
Our Species’ Best Medicine for Parenting a Baby Following a Cesarean
- Kangaroo Mother Care: Dr. Nils Bergman on Skin to Skin after a Cesarean
- Skin to Skin is Good For You Too: It Wires Your Brain for Post-Cesarean Parenting
- Separation is Stressful!
- What if my Baby and I are Separated?
- My Interview with Jill Bergman: Getting Practical about Skin to Skin after a Cesarean
- More Dr. Bergman (thebirthpause.com)
- Skin to Skin Carriers for Women and Men
- Benefits of Kangaroo Mother Care
Kangaroo Mother Care: Dr. Nils Bergman on Skin to Skin after a Cesarean
“Cesareans are good for many reasons,” says Nils Bergman, a South African physician and international promoter of Kangaroo Mother Care (KMC). “Yes, if medically indicated, cesarean is good. But the separation of a mother and her baby following a cesarean, now that is something altogether different.”[i]
Years ago in Zimbabwe, Dr. Nils Bergman introduced a protocol to keep low-weight preterm infants on their mothers, skin to skin, while every other aspect of care remained the same. He found that survival rates for these babies surged from 10 to 50 percent. Dr. Bergman later conducted a randomized controlled trial and found that preterm newborns in skin on skin contact with their mothers for the first six hours after birth were 100 percent stabilized. For babies in incubators, less than 50 percent had stabilized within six hours.[ii]
Dr. Bergman became convinced that on-going skin to skin contact is what our species expects at birth, reflecting millions of years of evolution, and yielding significant physical and emotional health benefits for babies and their parents. His findings have launched an international mother-baby skin to skin revolution. Dr. Bergman now lectures throughout the world about the neuroscience behind Kangaroo Mother Care. He is challenging health care providers and parents to comprehend what is normal for nature – and for our natures — regardless of what is normal for our Western culture.
For babies born by cesarean, Dr. Bergman considers skin to skin contact essential. He explains that infants born by cesarean do not experience the same post-birth spikes of important hormones such as norepinephrine that wakes the baby’s brain and activates pumping actions that clear the lungs of fluid. Additionally, mothers who birth by cesarean and babies born by cesarean have been shown to have lower levels of oxytocin than when babies are born vaginally.[iii] Dr. Bergman recommends that following a cesarean parents compensate for these lower hormone levels with continuous skin to skin and hourly breastfeeding.
Of course, sometimes there are unavoidable separations or stressful procedures a baby must endure. Dr. Bergman’s wife, doula and author Jill Bergman, says, “When separations occur, the question is how quickly can we restore the baby to what she anticipated with oxytocin-enhancing skin-to-skin and breastfeeding.” [iv]
While Kangaroo Mother Care just celebrated a major victory (six major international health associations endorsed the universal use of KMC for preterm and low birthweight infants), KMC is not yet a standard of care post-cesarean. Families may have to ask nurses and doctors to do things differently to assist with on-going skin to skin contact. Extra help may be needed from family, friends, a doula or KangaroulaSM (what is a kangaroula? Keep reading…) to make KMC happen in the sensitive hours, days and weeks following a cesarean.
“I watched, and after a few minutes, I could tell that the pediatrician was done with his procedures, so I asked if they could place him on me for skin to skin. Although the pediatrician had been prepped that this was the plan, he looked dumbfounded and said, ‘I’ve never done skin on skin in the operating room.’ My doctor stated confidently, ‘That’s what we’re doing!’ The nurse piped in, ‘I have!’ and whisked my son from the doctor and placed him on my chest.” Athena
“Charlie was in our arms for the first two days of life– we literally didn’t let the nurse take her for anything without one of us holding her! I really feel this helped her emerge into the world from a safe place.” Tiffany and Tom
Skin to Skin is Good for You Too: It Wires Your Brain for Post-Cesarean Parenting
Your baby anticipates skin to skin contact, but so too does your brain. During pregnancy, maternal hormones make new branches on neurons. Birth, then, is a time of great neural plasticity for mothers. Quite literally, experiences during the first hours and days after birth are wiring your brain for motherhood.
Breastfeeding and mother-infant contact lead to high oxytocin levels that positively activate changes in mothers’ brains. Following a cesarean birth, get help and do as much skin to skin as possible! Your mommy-brain will thank you.
Data show that in animal and human studies, high oxytocin interactions with babies (skin to skin and breastfeeding) result for mothers in improved:
- emotional fitness,
- boredom tolerance,
- stress tolerance,
- resilience,
- ferocity in defense of young, and
- reduced likelihood of post partum depression.[v]
As behavioral neurobiologist Sue Carter writes, “The role of natural oxytocin includes molecular pathways in the transition to motherhood such as buffering stress reactivity, supporting positive mood and regulating healthy mothering behaviors.” These changes create “a healthy, ‘protected’ brain that may provide benefits to its owner well into senescence.”[vi]
Dr. Bergman says the mother has to make a profound investment and her biology changes. “We have a window here,” he says, “for the first 1000 minutes, mother and baby are skin on skin, approximately two days wiring before she makes mature milk. The baby is altering the mother’s mind.”
And for fathers? Dr Bergman says that somewhere in the 1000 minutes 30-60 minutes are needed for the father’s wiring: “These fathers are profoundly and permanently altered for connection and protection.”
What’s not to love about skin to skin?

“Greg knew how important skin to skin contact was to me, so as soon as they handed him the baby in the operating room, he stuffed him into his scrubs, right onto his naked chest. The nurses were horrified he didn’t wear a shirt underneath but at least the baby got some of our bacteria!” Natasha
Separation is Stressful
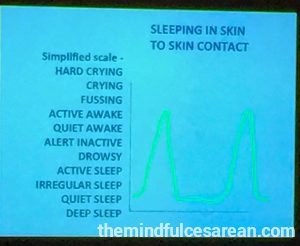
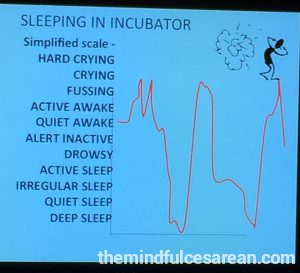
Dr. Bergman and his colleagues conducted a study to understand the effect of even short-term separation of a newborn from its mother. They measured deep sleep and heart rate variability (as an indicator of central anxious autonomic arousal) in two-day-old newborns as they slept skin-to-skin with their mothers and when they slept alone in a nearby crib. During the time the babies were separated from their mothers, the babies’ autonomic arousal averaged 176 percent higher and quiet sleep 86 percent lower than when they slept skin to skin with their mothers.[vii] “We made a startling discovery,” Dr. Bergman said. “When babies sleep separate from their mothers heart rate variability triples, deep sleep is significantly reduced, and there is no sleep cycling.” Furthermore, he said, “The absence of the mother, even for a short period, doubles cortisol for full term infants. In preterm NICU babies, cortisol is ten times higher for babies in incubators than for babies skin on skin.”
Dr. John Krystal, Chairman of the Department of Psychiatry at Yale, commented on the study’s findings: “This study highlights the profound impact of maternal separation on the infant. We knew that this was stressful, but the current study suggests that this is a major physiologic stressor for the infant.”[viii]
Keep your baby close!
![]()
“I am proud of my choice to bed share. I love snuggling with him all night. I don’t mind feeding him in the night because we are both half asleep when he nurses. He’s a great sleeper and I think it has something to do with the fact that he knows I am always there for him, even in the night. He is so strong, so passionate and growing so perfectly. I might not have gotten the natural birth that I wanted, but I am getting to be the natural mama I always longed to be.” Athena

What if My Baby and I are Separated?
If you and your baby experience a separation, make special time with your baby to reconnect. Put away all distractions and hold your baby skin to skin. Pay attention to your child. Explain why you had to be separated and reassure her that she is safe with you.
Midwife Karen Strange reminds parents that difficulties, separations, or disruptions in sequences happen; in fact, she says, they are inevitable. “I don’t know anyone with the perfect birth, the perfect childhood, the perfect adolescence, and the perfect marriage,” she says.
Perfect is not the point. Repair is. It is the coming back, the finding of each other again, that mends the separations. When things go less than swimmingly for our babies and children, we slow down for the reconnection. It doesn’t matter if a child is still in utero, newly born, or heading off to college. It is what we do with and for our children day after day, year after year, and our relationships are stronger than if there had been no ruptures.
At birth, when a baby has a stressful experience, Midwife Karen Strange says that repair will be found when mother and baby come together for a quiet, uninterrupted time where a baby is given the opportunity to do what she is born knowing how to do: bop and scooch her way to her mother’s breast, skin to skin. Karen emphasizes that repair is possible no matter if the repair happens minutes, hours, or even days or weeks after the birth. This coming together of mother and baby, she said, is an opportunity to heal the separation of birth and any disruptions in sequences that may have followed the birth and it can happen at any time. “Repair,” she says, “is always possible.”[ix]
Kangaroula Support? What’s that?
As Nils and Jill Bergman describe it, “Kangaroo Mother Care plus doula equals kangaroula!”
The work of the Bergman’s foundation, Neuroscience for Improved Neonatal Outcomes (ninobirth.org), conducts research into and advocates for conditions that support optimal brain development for babies at birth. Jill Bergman now also trains birth attendants to offer what she and Nils Bergman call KangaroulaSM care. Doulas trained in this approach understand the importance of skin to skin, breastfeeding and a low-stress birth environment for the health of mother and baby, and do their best to help families get off to a strong start, no matter the circumstances of the birth.
To gather practical tips on offering families Kangaroo Mother Care in the days and weeks after a cesarean, especially if extra medical attention is needed, I got in touch with Jill Bergman at her home in Cape Town, South Africa.
Kangaroo Mother Care with a Cesarean: Interview with Author and Doula Jill Bergman

Jill and Nils Bergman
Mary Esther: First of all, I would like to thank you and your husband, Dr. Nils Bergman, for the work you’ve done to promote skin to skin contact between mother and baby as a new—but of course very old—norm. When it comes to cesarean, you and Dr. Bergman are integrating what is biologically ancient—skin to skin—with our technologically new surgical births. I’d love to talk about how you support families to maximize Kangaroo Mother Care during and following a cesarean. To start, how would you describe the particular benefits of skin to skin contact during a cesarean?
Jill: Sure. In a vaginal birth, a baby comes from a warm, dark peaceful place with mum’s familiar voice, heartbeat and smell, into a normally brightly lit room with nurses and doctors and noise. This takes a lot of adjustment for the baby.
In a cesarean, the adjustments are even greater for a baby. The operating lights are acutely bright. The room smells of antiseptic and is colder than a regular delivery room. The baby may have had no preparation from contractions to prepare him for the birth, so the sudden transitions are even more scary for him. He is held by doctors with strange smelling plastic gloves, examined on a resuscitation table with extremely bright lights and then often routinely placed into a warm incubator and wheeled away to the nursery for “observation.” This is separation from everything that is familiar to the baby. This causes instability in the newborn.
However, if the baby is placed on mother’s chest while the mother is being sewn closed, mother’s familiar voice, heartbeat and smell will calm him. Her chest will warm him and he will stabilize physically much faster. The smell of colostrum will draw him to move towards the nipple and he will self-attach and start to breastfeed. In the strange operating environment, he has the “buffering protection of adult support.” The contact also helps the mother to bond with her baby. It helps her to be less anxious about the operation as she focuses on her baby on her chest. She can skip the worry of seeing her baby being wheeled away.
Mary Esther: Do you have any tips for how partners can help mothers hold their babies skin to skin in the operating room, even as the surgery is still underway?
Jill: Partners are very important. Partners can support by holding the baby on mum’s chest. Remember, mum’s one arm has a drip and the other has a blood pressure cuff. Partners can also check baby’s breathing and color and make sure he is covered by a blanket.
Mary Esther: Dr. Bergman discusses the importance of enhancing oxytocin for mother and baby for the first 1000 minutes after birth. Following a cesarean, a mother is in the first stages of recovering from surgery and simultaneously figuring out breastfeeding and how to parent her baby. What helps families keep babies skin to skin during this sometimes challenging time?
Jill: A mother recovering from a cesarean knows she has to look after her baby and this helps the recovery. All of her maternal instincts will be focused on her child. But she needs help. If she has just had a cesarean, she won’t be able to pick up her tiny newborn, so there needs to be someone to assist her, possibly her partner, another family member, or a doula we call a “kangaroula.” If both parents are allowed to stay in the unit for the first days, it is hugely helpful for the mother’s recovery as they share the load and work out together how to care for their baby. It makes father much more part of the family and care. Fathers have a special role to play as the baby can sleep on him without the stimulation of the smell of breastmilk. The baby is born, but in this way, the family is born too!
Mary Esther: You mentioned support by a doula known as a “kangaroula.” What is kangaroula care? How does a doula trained in this approach help make the time after the birth as oxytocin-rich as possible for mother and baby?
Jill: Doulas care for and support a mother in labor and focus on her needs. A kangaroula does this as well but is also a voice for the baby’s needs. For example, she might help a mother delay or avoid an epidural to minimize the transfer of drugs to the baby; she might help a woman avoid an unnecessary, planned cesarean since this is unexpected and stressful for the baby.
After the baby is born, a doula trained to offer kangaroula support will be thinking about the baby’s experience as well as the mother’s and do what she can to limit stress on the baby. She will dim the lights or cover the baby’s eyes, ask for quieter voices and set up a gentle environment for the baby and mother. Most of all, a kangaroula will advocate for the baby not to be separated from mother unnecessarily and will support undisturbed time for the first two golden hours to bond and start breastfeeding. A kangaroula will also help new parents transition to parenthood by helping parents understand ways to protect togetherness and minimize interferences in the days to come.
Mary Esther: There are many reasons why a baby born by cesarean might be taken to the NICU, some for observation and others for needed medical care. In most U.S. hospitals this means we now have a baby and mother who are separated, sometimes for days, with scheduled visits, every two to four hours, although sometimes more frequently. Usually skin to skin and breastfeeding are permitted and often encouraged during these visits, but the baby remains in the nursery while the mother stays in her recovery room or at home. Dr. Bergman speaks to this point directly, saying the incubator “is the wrong place for the baby. Incubators destabilize. We bring needed medical care to mother and baby whenever possible.”
Jill: Yes. Absolutely. The design of the NICU as a separate space from the maternity ward needs to be challenged as it makes the start of breastfeeding nearly impossible and negatively impacts early bonding. We need the baby on the mother’s chest nuzzling at the breast, stimulating breast milk production and the hormones that we know promote healthy bonding.
Mary Esther: Do you have any tips for parents who feel strongly about maximizing skin to skin contact if their baby is in a NICU in a typical U.S. hospital where separation is the norm and contact is scheduled, especially if medical attention is needed for the newborn?
Jill: Of course some babies need medical care. The answer is to bring the medical support to the right place: the mother’s chest. There is always room for a chair next to an incubator, even a fold-up deck chair so the mother can lean back and rest. We have to ask doctors to adapt their practices so that care is available to the baby on its mother’s chest.
Mary Esther: Change can come slowly to hospitals. What have you seen on this front in South Africa?
Jill: I’ve seen parents and doulas change hospital practices by asking questions and being assertive. I’m thinking of a father who politely refused to leave the recovery ward because his wife needed help with breastfeeding. Eventually they allowed him to stay and now they have put up more curtains between beds and fathers are permitted to stay. When I first asked OBGYN for permission to attend cesareans at one of our local hospitals five years ago as a doula, it was unheard of. Now partner and doula are allowed in routinely. But some hospitals are unbending. In those cases, it makes sense to switch hospitals if possible. I recently had a mum needing a third caesarean who phoned me at 40 weeks because she would not be allowed to hold her baby in the operating room, and her baby would be taken to NICU. We found another doctor and another hospital where she could breastfeed her baby in the operating room and remain together. She was very pleased with the change.
Mary Esther: Because women are usually on pain medication that can affect their mental clarity and alertness, hospital personnel are often concerned about women sleeping with their newborns on their chests in the days following a cesarean. They insist the mother place the swaddled infant in a nearby bassinet for sleep. Given what we are learning about how stressful this separation can be for a newborn how do you think about this issue?
Jill: Let’s keep in mind that the baby needs the smell of mother to sleep-cycle properly. The baby does need to be carefully observed and mum and baby should not be left alone. The baby can be tied on safely to the mother’s chest with the airway open. We have developed what we call a Kangacarrier for this purpose. This is what we do even for preterm babies. It makes a tremendous difference.
Mary Esther: When the family gets back home, what tips would you offer to support on-going skin to skin contact?
Jill: Get a carrier that is non-stretchy and carry your baby when you are home. Mothers can undress the baby and place her in skin to skin contact on her chest. Fathers can wear the baby too. Get lots of help so you can focus on the baby!
Mary Esther: I’d also like to ask you about small, frequent feeds. Dr. Bergman describes one- hour sleep cycles syncing up with one-hour feed cycles as what nature intended. We often think in terms of feeding a newborn every two to three hours and many NICUs invite moms to nurse every four hours.
Jill: Babies inside the mother are swallowing amniotic fluid every 40 to 60 minutes. After birth, the sleep cycle is about 60 minutes. When the baby is born, keep to this one-hour cycle. The size of a newborn’s stomach is only five ml which is about one teaspoon. But the baby needs this small amount every hour or so. This is very natural if you keep your baby close to you with lots of skin to skin contact. With frequent feeds that follow the sleep cycle, the baby will learn food security as she sleeps and wakes and nuzzles on the breast and feeds and
falls back asleep.
Mary Esther: If a separation does happen, do you have any tips for reconnecting and recovering from the separation?
Jill: Yes. If a separation has happened, the question we can ask is “how quickly can we get mum and baby together again?” As soon as that happens, undress the baby and m

Jill Bergman, lower right, after her “Kangaroola” Training, Brooklyn, NY
other’s chest and let them lie together for hours, giving the baby a chance to go through the wriggling and nuzzling towards the breast. Let the baby latch supported, but undisturbed, for as long as it takes for both of them to calm and settle and be together, even for days. This is healing for both of them!
Mary Esther: Thank you so much, Jill.
Jill Bergman has been involved with Dr. Nils Bergman in supporting and promoting Kangaroo Mother Care for 25 years. As a teacher and counselor she wants all parents to be given the neuroscience of caring for their newborn babies in normal non-medical English. She has written and produced four DVDs on KMC and written a book called “Hold Your Premie,” a practical workbook on skin-to-skin contact for parents of premature babies. Jill is a qualified DOULA, and her knowledge of developmental care, and the neuroscience on KANGARoo Mother Care, makes her a unique advocate for the baby at birth, a KANGAROULA! She can be reached at jill@ninobirth.org
Dr. Nils Bergman calls himself a public health physician and currently promotes and researches skin-to-skin contact on a full-time basis. He is an honorary research associate and honorary senior lecturer at the University of Cape Town, South Africa. Dr. Bergman was born in Sweden and raised in Zimbabwe, where he also later worked as a mission doctor. He received his medical degree at the University of Cape Town and later a Masters in Public Health at the University of the Western Cape. His last posting was senior superintendent of Mowbray Maternity Hospital in Cape Town, overseeing 18,000 births per year. He enjoys sharing the wildlife of Africa with his wife, Jill, and their three children. Nils can be reached at nils@kangaroomothercare.com

from left to right: Mary Esther Malloy, Nils Bergman, Annette Perel, Bonu deCaires
Mary Esther Malloy holds a MA in anthropology. She is a doula, Bradley educator, and mother of three children who writes frequently about birth. You will find additional articles and recordings by Mary Esther at mindfulbirthny.com. If you are interested in the neuroscience of skin to skin and breastfeeding, she invites you to visit her blog thebirthpause.com where you will find her popular post “Kangaroology: The First 1000 Minutes” about Dr. Nils Bergman’s 2016 talk at NYU. Mary Esther is proud to announce that she recently certified with Jill Bergman to offer KangaroulaSM Care. She can be reached at info@mindfulbirthny.com
More Dr. Bergman: The Neuroscience of Skin to Skin and Breastfeeding
“Kangaroology: The First 1000 Minutes”
For more on the neuroscience of skin to skin, see my blog post about Dr. Bergman’s 2016 lecture at New York University. thebirthpause.com
Skin to Skin Carriers for Women and Men
There are now many skin to skin carriers on the market which make caring for your baby on your body much easier.
The Kangacarrier!
The skin to skin carrier that got it all started: the Bergman’s Kangacarrier. This carrier is appropriate for stabilizing an unstable preterm and excellent for full term babies as well. Women and men wear these carriers. Their tie-on approach is what the Bergmans have used in their South African hospitals to safely keep mother and baby together night and day following a cesarean (or any birth). www.ninobirth.com

Jill Bergman tying a baby doll on doula Chantal Traub as part of NINO’s Kangaroula Support Training, Brooklyn, NY

Nils Bergman describing how the Kangacarrier is used, Brooklyn, NY
Nesting Days
Here is my friend wearing a Nesting Days sling with her preterm infant son. (Thanks to the New York Milk Bank and generous NYC mamas, he has had nothing but breastmilk!) nestingdays.com

New mom, Laura Wolfe, modeling her much-loved Nesting Days carrier, NY, NY
Vija Design
Vija Design has nice skin to skin carriers for mothers and fathers. Vija-designs.com

New dad, Kyle Fabel, sporting a Vija-Design Dad’s Skin to Skin Carrier

New dad, Matthew Taylor, modeling his new skin to skin carrier (as cool as the dad in the ad, no question!)

Hands free Dad!
Please let me know about others you love!
The Benefits of Kangaroo Mother Care (Skin to Skin)
Adapted from ICEA Position Paper, “Skin to Skin Contact”
Research has shown that with immediate skin to skin contact following the birth we have:
- Temperature regulation;
- cardio-respiratory stability;

- self-attachment for breastfeeding;
- higher blood glucose levels;
- infant’s hands & feet warmed within 90 minutes of initiating skin to skin care;
- better breastfeeding compared to incubator care (twice as likely);
- shorter length of stay in the NICU.
Studies demonstrate that skin to skin contact in the postpartum period benefits both mother and baby:
- infant cries 10 times less and for shorter periods than infants in cribs;
- increased maternal affectionate/nurturing behaviors;
- enhances effective breastfeeding;
- mother’s sleep synchronized with newborn;
- apnea reduction;
- less initial weight loss;
- better state organization (moving from sleep to awake & back) and motor system modulation (smoothness of movement);
- more restful natural sleep cycles and more quiet sleep;
- reduced stress reaction to painful procedures.
Research indicates many long term benefits of on-going Kangaroo Mother Care for infants and children:
- fewer infections at 6 & 12 months;
- smiles more often at 3 months;
- ahead in social, linguistic, fine/gross motor indices at 1 year;
- earlier urinary continence;
- earlier stubbornness;
- mothers & children were smiling and laughing more in free play;
- mothers more encouraging and instructing towards children;
- improved brain maturation;
- enhanced self-regulation;
- better emotional and cognitive regulatory abilities and more efficient arousal at 3 & 6 months;
- improved attachment.[x]
[i] Dr. Nils Bergman lecture at New York University, New York, February 2016. For more from this lecture visit my blog thebirthpause.com “Kangaroology: The First 1000 Minutes.”
[ii] Nils Bergman, A Jurisoo, “The ‘kangaroo-method’ for treating low birth weight babies in a developing country,” Tropical Doctor 24, (April 1994): 57-60.
[iii] James E. Swain, Esra Tasgin, Linda C. Mayes, Ruth Feldman, R. Todd Constable, and James F. Leckman, “Maternal brain response to own baby-cry is affected by cesarean section delivery,” J Child Psychol Psychiatry 49, no.10 (2008 Oct):1042-52
[iv] Jill Bergman lecture at Birth Day Presence, New York, New York, October 2016
[v] Ann Bigelow, Michelle Power, Janis MacLellan-Peters, Marion Alex and Claudette McDonald, “Effect of mother/infant skin-to-skin contact on postpartum Depressive symptoms and maternal physiological stress,” Journal of Obstetric, Gynecologic, & Neonatal Nursing
41, Issue 3 (May/June 2012): 369–382.
CH Kinsley, KG Lambert, “Reproduction-induced neuroplasticity: natural behavioural and neuronal alternations associated with the production and care of offspring,” J Neuroendocrinol 20 no. 4 (April 2008): 515-25. 2008
GI Leng, SL Meddle, AJ Douglas, “Oxytocin and the maternal brain,” Curr Opin Pharmacol 8 no.6 (Dec 2008):731-4.
AF Bell, EN Erickson, CS Carter, “Beyond labor: the role of natural and synthetic oxytocin in the transition to motherhood,” Journal of Midwifery & Women’s Health 59, no.1, (2014): 35–42.
[vi] Kinsley and Lambert, p. 517.
[vii] BE Morgan, AR Horn, NJ Bergman, “Should neonates sleep alone?” Biol Psychiatry 70, no.9 (2011):817-25.
[viii] “Maternal separation stresses the baby,” Research and journals: Elesevier (2011).
[ix] Mary Esther Malloy, “New science new practices: slowing down at birth for vulnerable newborns,” Journal of Prenatal and Perinatal Psychology and Health 30, no.2 (Winter 2015):122-135.
[x] ICEA Position Paper, “Skin to skin contact,” (n.d.). Retrieved at
http://icea.org/sites/default/files/Skin%20to%20Skin%20Contact%20PP-FINAL.pdf, June 2014.

